Fill Your Medication Administration Record Sheet Template
Fill Your Medication Administration Record Sheet Template
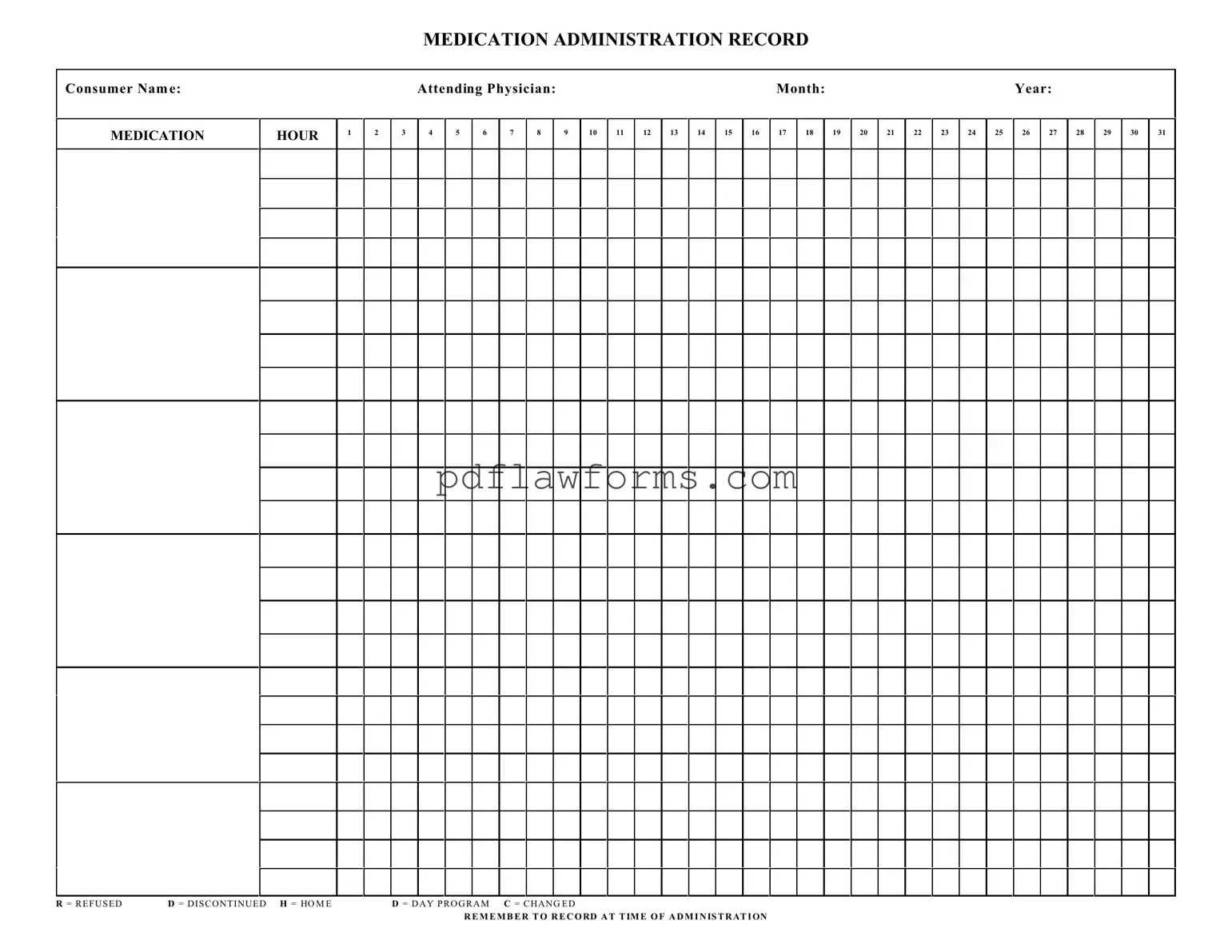
The Medication Administration Record Sheet (MARS) is an essential tool used in healthcare settings to ensure that patients receive their medications accurately and on time. This form includes critical information such as the consumer's name, the attending physician, and the specific month and year of administration. Each day of the month is represented, allowing healthcare providers to track medication administration for up to 31 days. The form also features designated columns for recording the time of administration, making it easy to note when a medication is given. In addition to the standard entries, there are specific codes to indicate various situations: 'R' for refused, 'D' for discontinued, 'H' for home, 'D' for day program, and 'C' for changed. These notations help maintain clear communication among healthcare staff and ensure that any changes in a patient’s medication regimen are documented promptly. By keeping accurate records, healthcare providers can better manage patient care and adhere to safety protocols.
Understanding the Medication Administration Record Sheet (MARS) is crucial for ensuring proper medication management. However, several misconceptions can lead to confusion. Below are ten common misconceptions about this important form, along with clarifications.
By addressing these misconceptions, staff can enhance their understanding of the Medication Administration Record Sheet, leading to improved patient care and safety.
Filling out a Medication Administration Record Sheet can be a straightforward process, but several common mistakes can lead to confusion or errors in medication management. One frequent error occurs when the consumer's name is not clearly written. This can result in miscommunication among staff members and potentially jeopardize patient safety. Always ensure that the name is legible and correctly spelled.
Another mistake is failing to record the correct date. The month and year must be accurate to ensure that medications are administered as per the prescribed schedule. An incorrect date can lead to missed doses or administering outdated medications, which could have serious health implications.
Many individuals overlook the importance of documenting the time of administration. Each medication should be recorded at the exact time it is given. This practice helps track adherence to the medication schedule and can alert healthcare providers to any patterns of refusal or missed doses.
Inconsistent use of abbreviations can also create confusion. For instance, using different symbols for the same action—like "R" for refused and "D" for discontinued—can lead to misunderstandings. It is essential to use standardized abbreviations consistently throughout the form to maintain clarity.
Some people neglect to check the attending physician's name, which should be included on the form. This detail is crucial for accountability and ensures that any questions about the medication can be directed to the right person.
Another common oversight is failing to indicate any changes in medication. If a medication has been altered, such as a dosage change, it should be clearly marked on the record. This practice ensures that all staff are aware of the current treatment plan and can provide appropriate care.
Lastly, many individuals forget to sign the record after completing the medication administration. A signature not only confirms that the medication was given but also serves as a legal record of compliance with medication protocols. Always remember to sign and date the record to uphold accountability and transparency.
Filling out the Medication Administration Record Sheet is essential for tracking medication given to consumers. This ensures that each individual receives their medications accurately and on time. Follow these steps carefully to complete the form.
Fillable Da Form 638 - All entries must be accurate to facilitate the approval process.
The Virginia Motor Vehicle Bill of Sale form serves as a vital document that facilitates the transfer of ownership of a vehicle between a seller and a buyer. For those looking to ensure they have the correct paperwork, resources like My PDF Forms can provide the necessary templates and guidance, enhancing the security and efficiency of the transaction.
Edd Disability Form - The DE 2501 form must be signed before submission to validate the information provided.