Fill Your Cna Shower Sheets Template
Fill Your Cna Shower Sheets Template
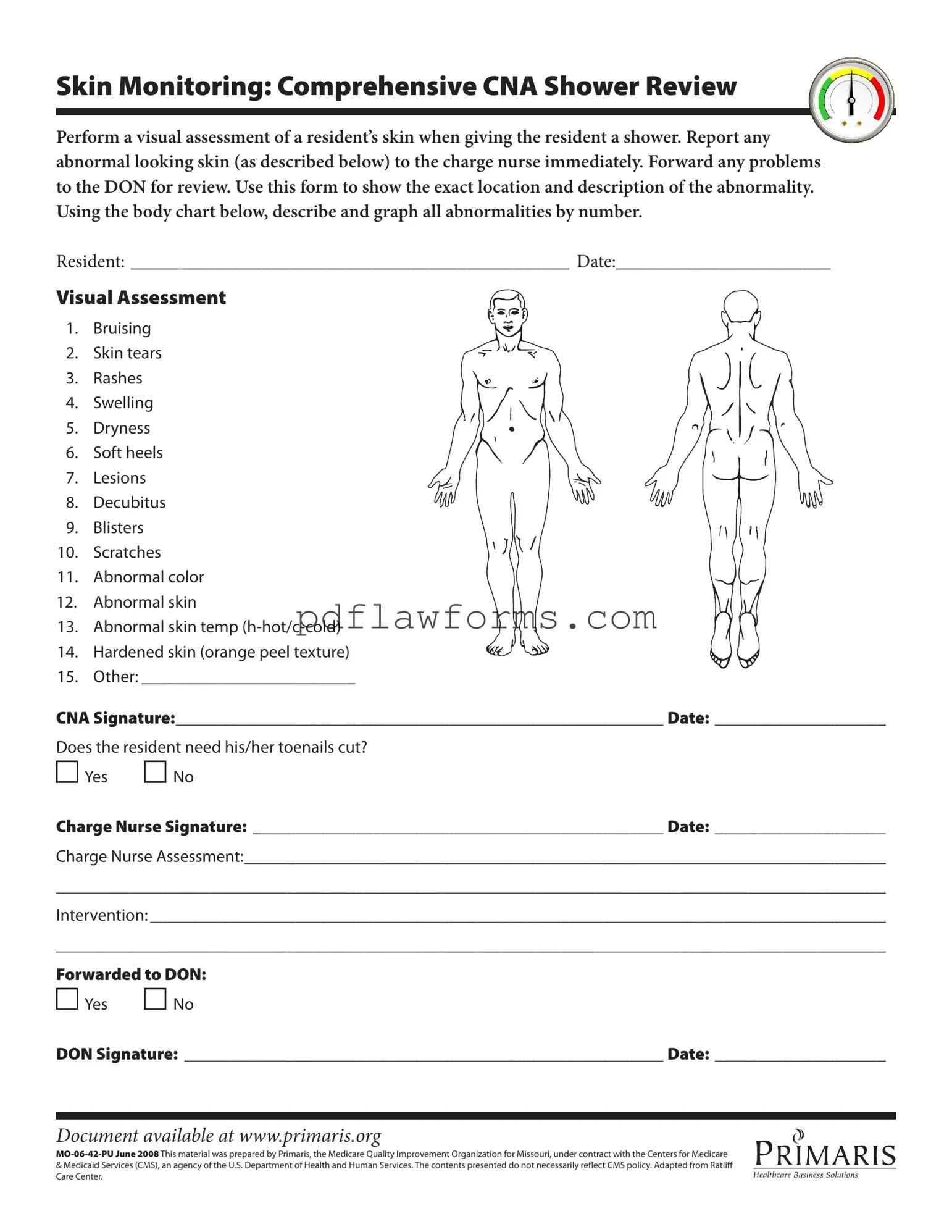
The CNA Shower Sheets form is a vital tool for ensuring the health and safety of residents during their bathing routines. This form facilitates a thorough visual assessment of a resident's skin while they are receiving a shower. It is essential for Certified Nursing Assistants (CNAs) to document any skin abnormalities such as bruising, rashes, or lesions, as these could indicate underlying health issues. Upon identifying any irregularities, CNAs are required to report their findings immediately to the charge nurse and subsequently forward any significant concerns to the Director of Nursing (DON) for further review. The form includes a body chart where CNAs can accurately pinpoint and describe the location of each abnormality. Additionally, it prompts the CNA to assess other needs, such as whether the resident requires toenail trimming. By signing the form, CNAs affirm their observations, while the charge nurse's signature indicates that an assessment has been conducted. This collaborative approach not only promotes effective communication among staff but also prioritizes the well-being of the residents. Overall, the CNA Shower Sheets form is an integral component of resident care, ensuring that any potential skin issues are promptly addressed and monitored.
Misconceptions about the CNA Shower Sheets form can lead to misunderstandings in its use and purpose. Here are seven common misconceptions, along with clarifications:
Understanding these misconceptions can enhance the effectiveness of the CNA Shower Sheets form, ultimately improving resident care.
Filling out the CNA Shower Sheets form accurately is crucial for proper skin monitoring and care. However, many people make common mistakes that can lead to misunderstandings or inadequate care. One significant error is failing to provide the resident's name and date at the top of the form. Without this information, it becomes difficult to track the resident’s care history.
Another frequent mistake involves not performing a thorough visual assessment. Some CNAs may rush through the shower process and overlook important signs of skin abnormalities. It is essential to take the time needed to assess the skin properly. Missing details such as bruising or skin tears can result in untreated conditions.
In addition, CNAs sometimes neglect to describe the abnormalities clearly. Using vague terms or omitting descriptions can lead to confusion. Instead, specific details about the size, color, and location of the issues should be documented. This clarity is vital for the charge nurse and the Director of Nursing (DON) to understand the situation accurately.
Another common error is failing to mark the abnormalities on the body chart provided. This chart is a visual tool that helps identify the exact locations of issues. Not utilizing it can lead to miscommunication and oversight in treatment. Each abnormality should be numbered and clearly indicated on the chart.
Some CNAs also forget to check the box regarding whether the resident needs toenail care. This simple step is often overlooked but is important for the resident’s overall hygiene and comfort. Neglecting this detail can lead to discomfort or further complications for the resident.
Inaccurate signatures can also pose problems. The CNA must sign and date the form correctly. If the signature is illegible or missing, it may raise questions about who completed the assessment. This issue can complicate accountability and follow-up care.
Additionally, CNAs may fail to report abnormalities to the charge nurse immediately. Timely reporting is critical in ensuring that any issues are addressed promptly. Delaying this communication can lead to further complications for the resident.
Some CNAs do not forward the completed form to the DON, which is another mistake. This step is essential for ensuring that all skin issues are reviewed and documented properly. Not forwarding the form can result in missed opportunities for necessary interventions.
Finally, some CNAs may overlook the importance of the charge nurse’s assessment section. This section is vital for documenting the charge nurse's observations and recommendations. Failing to fill it out can leave gaps in the care process.
By avoiding these common mistakes, CNAs can ensure that the CNA Shower Sheets form is filled out accurately and effectively, leading to better care for residents.
Filling out the CNA Shower Sheets form is an important task that ensures proper documentation of a resident's skin condition during showers. Accurate completion of this form helps in identifying any issues that may require further attention from nursing staff. Follow these steps carefully to ensure that all necessary information is recorded.
Dollar Sheet Fundraiser - This form allows members of the community to contribute a dollar to a local fundraiser.
The Florida Motor Vehicle Bill of Sale form is vital in the vehicle transaction process, ensuring that both the seller and buyer have a clear record of the details surrounding the sale. This official document not only captures the vehicle's description and purchase price but also includes personal information about both parties involved. For those looking for a convenient option to create this essential document, you can access it online at https://floridaformspdf.com/printable-motor-vehicle-bill-of-sale-form/, which provides a straightforward format for a smooth and legal ownership transfer required for vehicle registration in Florida.
Esa Papers - The documentation is often tailored to the individual’s unique circumstances.